
A Primer on Clinical AI 🏥
Close to 1,500 FDA-approved AI use cases, meta-analyses proving cost-effectiveness, and hospitals still aren't adopting.

Welcome back to Kiin Bio Weekly.
This week we’re looking at clinical AI, specifically the type that nobody’s talking about. I got connected to Ignacio through his work at Savana, where they’ve been extracting real-world evidence from clinical records for years. What struck me the most was how much of the conversation around AI in medicine misses the point: everyone’s focused on ChatGPT and scribes, while the predictive models that actually enable personalised medicine are sitting there with regulatory approval and population-level evidence, largely unused.
We got on a call, and the result is this primer.
Freebie alert: We know how hard science is. That’s why we built the Pioneer Programme.
We’re selecting academic and nonprofit research teams to get one year of free access to our drug discovery platform plus hands-on support from our science team. If your research bottleneck isn’t data but connecting the findings you already have, this is for you.
We’re looking for teams asking: which targets should we prioritise? How do we interpret conflicting evidence across datasets? Which hypotheses are worth testing next? Where are the strongest translational opportunities?
No cost. No data transfer. All IP stays with your institution. Applications close August, cohort starts September.

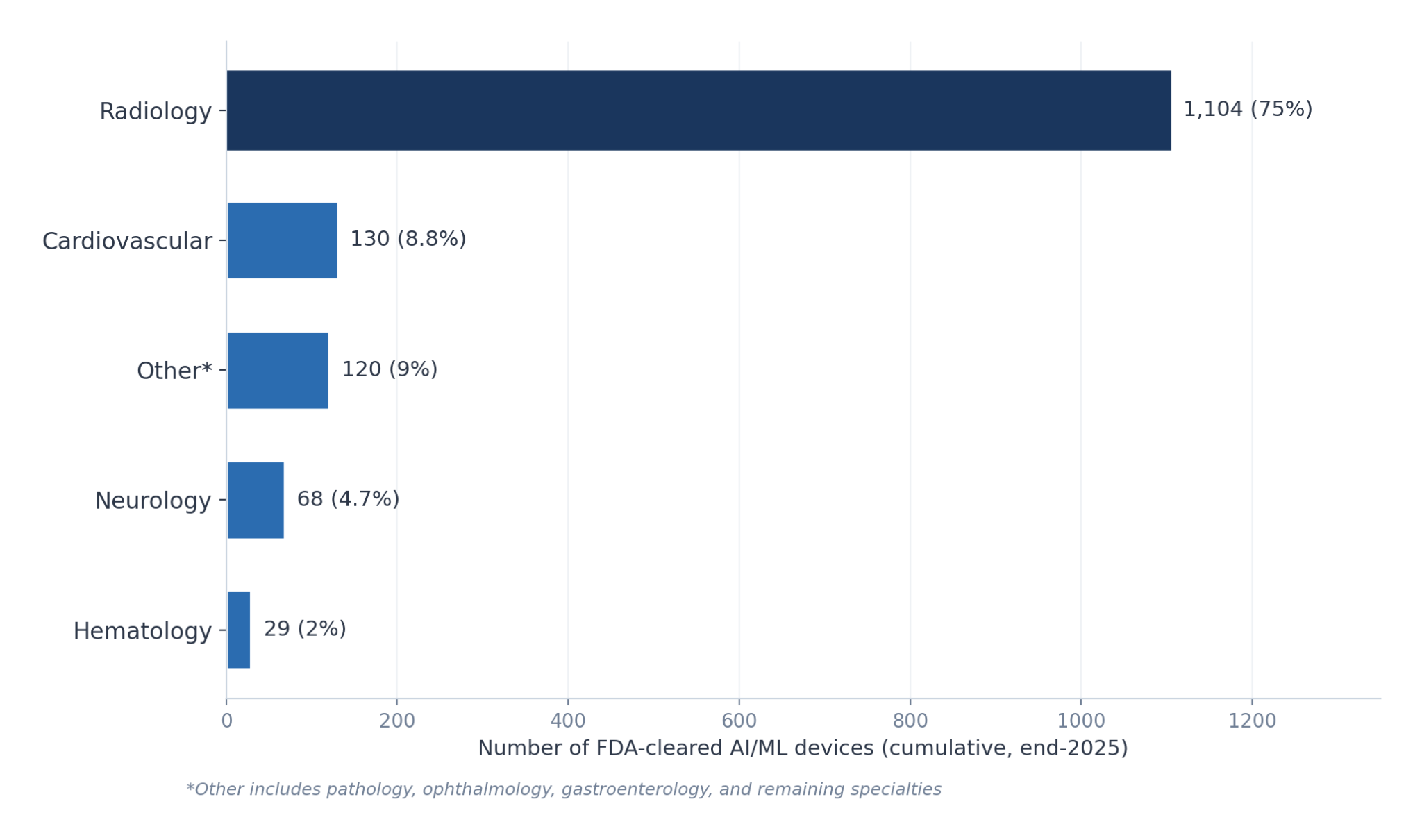
Healthcare systems across Europe are breaking. Waiting lists stretch to 14 months. The UK Health Secretary declared the NHS “broken.” Spain is close behind. Populations are ageing, medicines are expensive, and the workforce cannot scale. Into this crisis arrives artificial intelligence, not as a future promise, but as a present reality. The FDA has approved close to 1,500 AI use cases across clinical specialties. Meta-analyses now demonstrate cost-effectiveness in diabetes, colon cancer, and mammography screening. The question is no longer whether AI works in medicine. It is why adoption remains so slow.
Yet most clinicians, when asked about AI, will talk about ChatGPT and medical scribes. They are looking at the louder revolution while the quieter, more consequential one unfolds beneath it.
We spoke to Ignacio H. Medrano, neurologist-turned-CEO of Savana, about the real state of clinical AI: what is proven, what is hype, and what clinicians are getting wrong about the pace of change.

Ignacio H. Medrano, CEO of Savana
“It’s unethical not to use AI these days in certain areas, because it’s proven, and it’s proven at scale across populations.”
🔀 Two types of AI, one common misunderstanding
The most pervasive misconception among clinicians today is that generative AI (LLMs, chatbots, multi-modal models) is the only AI that matters. It is visible, fast-moving, and immediately useful: scribes that eliminate documentation burden, literature tools like Open Evidence replacing PubMed searches, agents managing waiting lists. These applications are exploding because they save time and, critically, do not require clinical validation. They handle documentation, not decisions.
But the deeper disruption is discriminative AI: predictive, classification-based models that have existed for over a decade. This is the AI that enables precision medicine. Granular predictions for individual patients about immunotherapy response, relapse probability in multiple sclerosis, optimal drug sequencing in haematologic cancers. It takes statistics to a level where you can determine the actual probability of a specific outcome for a specific patient.
Discriminative AI started earlier but arrives later in practice. Every algorithm requires validation, external replication, meta-analysis, and integration into clinical guidelines. That pipeline is slow. But it is the pipeline that delivers personalised medicine, and it is now producing results.
“A big misconception is forgetting that discriminative, predictive AI is the real silent disruption,” says Medrano. “The other is underestimating the speed at which agentic AI is arriving. People think this takes 20 years. It’s happening now, like thunder.”
✅ Separating signal from noise: what makes clinical AI “real”
With close to 1,500 FDA-approved AI applications and an exponential curve of machine learning publications on PubMed, distinguishing proven tools from hype requires a framework.
Medrano uses three levels:
Regulatory approval: FDA or EMA clearance confirms correct dataset construction, generalisation to new cohorts, and absence of bias. This is the minimum threshold.
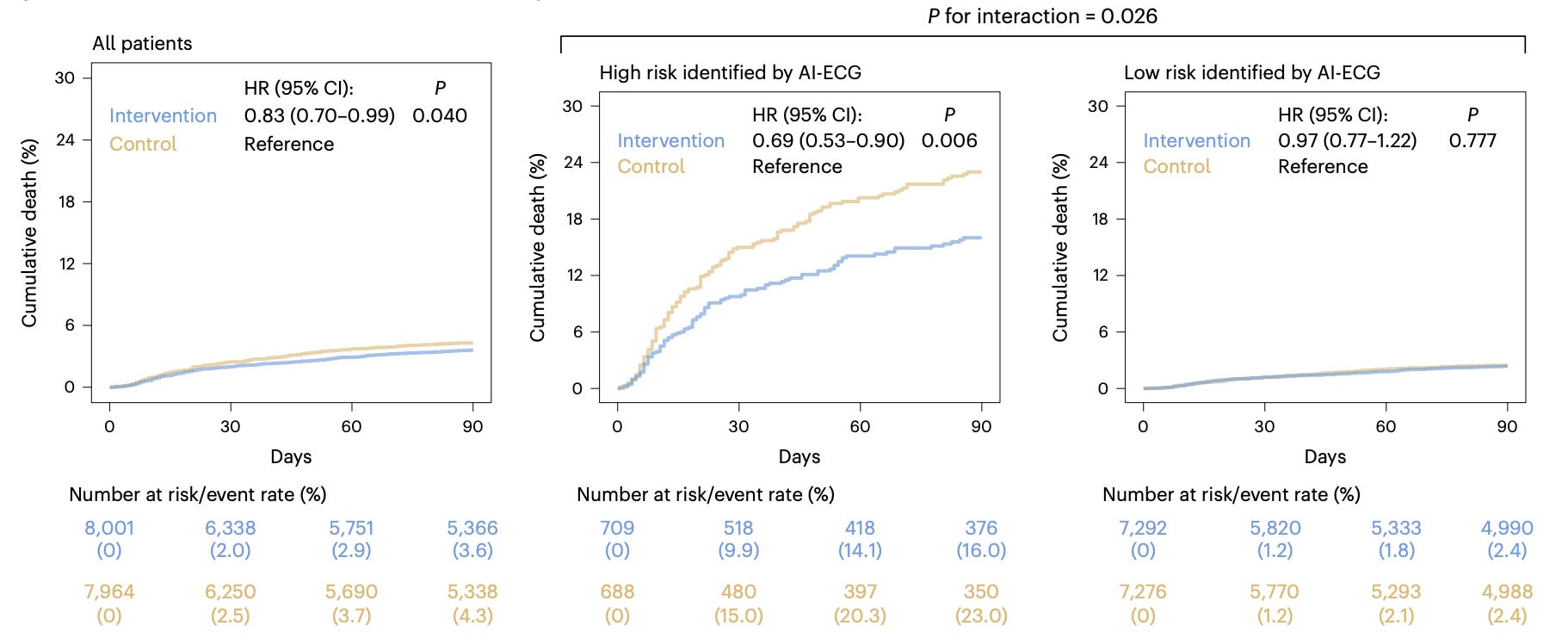
Population-level evidence: Publications demonstrating that algorithms work in general populations and are cost-effective. Meta-analyses now exist for AI in diabetes management, colon cancer screening, and mammography. A National Library of Medicine study proved chatbots reduce severe mental health events. A cardiology trial demonstrated that AI applied to ECGs reduces cardiovascular mortality.
Real-world deployment: Hospitals actually running these systems in clinical workflows. Hospital Clinic Barcelona has used AI to predict sepsis in intensive care for over three years. Finland deploys predictive models on GP workstations for population segmentation. In China, Ping An Good Doctor attends 100 patients daily without human involvement. In Utah, AI autonomously renews prescriptions.
The gap between levels two and three, between proven effectiveness and actual deployment, is where the real problem lives.
🚧 Three barriers, one that matters most
Technical: Clinical information remains fragmented across systems. Standards like HL7 FHIR are improving interoperability, but the problem is not fully solved. Training and validating models still requires stitching together disparate data sources.
Regulatory: Largely resolved. European regulation now recognises that anonymised data used for research does not require individual informed consent. The European Health Data Space will mandate hospitals to share data within one to two years. Countries like Switzerland, France, Germany, and the UK already permit compliant secondary use of clinical data.
Cultural: The real bottleneck. Not rejection; most managers and clinicians accept AI is inevitable. The problem is twofold. First, pure ignorance: hospital managers do not realise they could build pharmacogenomic models today that predict which patients will respond to expensive biologics, saving millions by paying only for drugs that will work. Second, politics: an algorithm that reduces the need for human labour is nearly impossible to sell when unions and the public demand 10 new nurses before any technology investment. Politicians choose nurses even when they understand AI’s value.
“It’s not belief anymore, it’s knowledge,” says Medrano. “Managers just don’t understand the power of what’s already possible with the data they have.”
📊 Real-world evidence: from luxury to necessity
Real-world evidence has always mattered. It is the difference between reading about a country and landing there. Clinical trials tell you what should happen under controlled conditions. Real-world evidence tells you what actually happens.
The barrier was always collection. Patient by patient, variable by variable, manually assembling registries over years. Exhausting, expensive, and therefore underutilised. Now, computational systems can extract this information automatically, reliably, and at scale from electronic health records. Once extraction became feasible, demand exploded. Regulators began requesting it. Pharma began requiring it.
This is where initiatives like the UK’s Foresight programme become significant: 57 million medical records feeding predictive models for 100 diseases at 20-year horizons. The Scandinavian countries (Norway and Denmark) are sharing data internationally and validating models across borders. These are not pilots. They are national-scale infrastructure decisions.
🤖 The convergence: agentic AI meets predictive models
Here is where the field is heading, and where most clinicians have not yet looked. The users of sophisticated discriminative AI models (multi-modal predictive algorithms trained on clinical text, genomics, proteomics, radiomics) will not be human doctors. They will be certified agentic AI systems.
Generative AI agents will orchestrate clinical workflows. Discriminative AI will provide the predictions those agents act on. The agent decides what to ask; the predictive model provides the answer. The human clinician supervises, validates, and handles what requires physical presence.
A meta-analysis of 15 studies already shows that in 13 out of 15, AI chatbots were rated as more empathic than human clinicians. Not even communication, the last presumed advantage of human clinicians, remains unchallenged.
“If doctors keep doing the same thing, they’ll become pointless,” says Medrano. “People will turn to their phones, where an agentic AI healthcare service for 10 euros will give them advice, pull their data, run algorithms. And then that agent will hire humans to perform the physical tasks it cannot.”
⚡ Where this leaves us
The infrastructure is being built. Data-sharing mandates are arriving. Validation evidence is accumulating. The two types of AI, generative and discriminative, are converging toward agentic systems that will reshape how healthcare is delivered.
The bottleneck is not technology or regulation. It is the speed at which institutions recognise what is already possible, and act before the system breaks entirely, or before patients simply route around it.
Big thanks Ignacio for meeting with us and sharing his insights for this primer!
💬 Want to be featured in Kiin Bio Weekly?
Each issue we speak directly with researchers, scientists, and builders working at the frontier of AI in life sciences. If you're working on something in this space and think it would resonate with our community, I'd love to hear from you. Fill out this form or reach out to me directly.
Found this useful? Forward it to a colleague in drug discovery or computational chemistry, it's the best way to help the newsletter grow.
Subscribe now to stay at the forefront of AI in Life Science. Every week: primers, deep dives, and direct conversations with the people building the field.
Connect With Us
Have questions on this or suggestions for our next deep dive? We’d love to hear from you!
📧 Email Us | 📲 Follow on LinkedIn | 🌐 Visit Our Website
Woah!! Thanks for the new information!!